Public Resources
Procedures
Hymenoplasty Surgery
“The hymen has a vast variety of appearances and will appear differently in the same person at different times of their lives and, between individuals at the same age. Despite persisting cultural mythology, it is not actually possible to determine if a woman is a virgin based on the state of her hymen. An intact hymen is regarded in many cultures as evidence of virginity where no assessment or requirement of male virginity is required. I perform hymen restoration for cultural reasons. For women caught between the traditions of their past and the reality of their lives today, this procedure may offer an alternative to dishonour, or even death. Hymen reduction is less controversial, but I apply the same degree of expertise and skill to produce a vaginal entrance, scar free, comfortable for intercourse, and looks normal.”
What is the hymen?
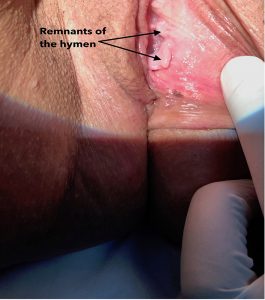
The hymen is a membranous structure that tends to cover the lower 2/3rds of the vaginal entrance. It is not universally present in all women and, rarely, the hymen may form to completely cover the vaginal introitus. The hymen can be present in many different forms; perforated, torn, irregular, a single sheet, thin and thick. Whilst usually delicate, the hymen can sometimes present as being very thick and relatively inelastic. Even in these cases, there are usually fine perforations in the membrane that allow the passage of menstrual blood. If the membrane completely covers the vaginal introitus and does not have any perforating passages, this is referred to as an imperforate hymen. The hymen can break or tear, spontaneously or during exercise, digital penetration of the vagina, use of a tampon, surgery.
What is hymenoplasty?
Hymenoplasty can either mean repair (restoration/reconstruction) or reduction of the hymen or hymenal remnants.
Patient perspectives
“I am from India and most people here think a girl having sex before marriage or with anyone other than husband is an unpardonable crime, which now I have committed and am not bold enough to let my fiancée know about this. In any case he will know when we get married and that would immediately cause disastrous effect on our marriage and may even lead to divorce. Please help me.”
“I have these things sticking out of my vagina. It doesn’t look normal and it’s really annoying during sex; rubs.”

Why do women requests hymen reduction?
In my practice I have noted 4 main reasons for women to request reduction of the hymenal tissues:
- Painful sex
- Hymenal remnants that either elongate or become thicker can result in painful intercourse as a function of the irritation of the hymenal tissue. Ongoing contact stimulation of this tissue results in hypertrophy and increased symptoms that, in some women, may result in avoidance behaviour
- Irritation at the vaginal entrance
- Hymenal tags can become thicker and longer as they continue to rub against the inner and outer parts of the vagina. When moving in and out of the introitus this can result in introital or vulval irritation. Chronic irritation can result from ongoing movement over a prolonged period.
- Aesthetic concerns
- Women may become aware of a change in the introital vaginal tissues after inspecting themselves, comments from a partner or feeling something that they had not noted to have been previously present. Not all women will be bothered by the visual changes unless they have physical symptoms. Others will have the impression that the vagina has changed and looks abnormal.
- Vaginal discharge
- Hymenal remnants that hypertrophy and elongate have a greater surface area, and this, combined with increased physical stimulation can produce an increase in vaginal introital discharge. This may be more symptomatic for some women at lower volumes than a ‘normal’ vaginal discharge because the discharge, occurring at the introitus appears more easily external to the vagina.
Dr Oseka Onuma is an expert hymenoplasty surgeon. When restoration is performed, his technique leaves no trace of surgery having been performed. Confidentiality is a key part of his practice. Your information remains private. When the hymen is reduced his skill and experience reduces the risk of scar tissue and leaves a natural, aesthetic appearance to the vaginal entrance.
For more information please do not hesitate to contact the office. Please request a confidential telephone discussion with Dr Onuma if required.
Book a ConsultationExcellence in Form and Function. Prevent, Treat and Maintain.
Labiaplasty Surgery
“Labiaplasty is increasingly topical, often contentious, challenging in unexpected ways, and emotive. As with all surgery, labiaplasty performed on a well-motivated, well-informed patient by an experienced, well-trained surgeon is preferred. My book, ‘So, you want a labiaplasty’ addresses the current scarcity of detailed information for women considering labiaplasty. I believe that it is essential reading for women considering surgery.
What are the labia?
- Labia minora
- Lying just outside the vaginal entrance are the labia minora. These are usually thin pieces of skin that do not contain fat or hair follicles. They extend up to and around the clitoris. Below, they can reach and extend around the forchette (lower part of the vaginal entrance).
- Labia majora
- The labia majora extend from the mons pubis above to the perineal area below. The inner leg forms the outer junction and the labia minora the inside junction. The outer surface is covered with pigmented skin, sebaceous glands, and after puberty, coarse hair. Beneath the skin there is mostly fatty tissue with some ligaments, smooth muscle fibres, nerves, and blood vessels.
Alternative names for labiaplasty include:
- Labioplasty
- Labia minora reduction
- Labia majora reduction
- Nymphoplasty
- Labial reduction
- Labia majorplasty
- Labia minorplasty
- Labia majora augmentation
What is labiaplasty?
Labiaplasty can be defined as surgery to change the shape of any part of the labia, typically making them smaller and/or correcting any asymmetry between them.
Labia minora reduction is the most requested surgery on the female external genitalia.
Patient perspectives
“I have great discomfort with my labial minora; they are both painful and embarrassing. The pain occurs from clothing and movement because they are so long. There is much discomfort when walking or sitting if they are not ‘tucked away’. I have also found sexual activities a great challenge and have not let anybody see or touch my vagina because of my labial minora.”

“Everything rubs on the labia. I have always had ample labia. Meaty. I have to wear pads every day but sometimes I’d prefer not to wear underwear or to just wear some lingerie. I also want it to look nicer and to be more comfortable.”

Why do women requests labiaplasty?
In my practice the main reasons for women to request labiaplasty are:
- 1. Functional
- Localised swelling of the labia due to friction
- Labia minora against labia minora
- Labia minora against labia majora
- Labia minora against clothing
- 2. Pain and/or discomfort
- During sporting activities such as cycling, running, gym work and horse riding
- When wearing tight clothes such as jeans or underwear
- Discomfort or difficulty when trying to insert a tampon
- 3. Cosmetic
- Unhappy with the way the labia look
- Impression that they look abnormal
- Worried because they look different to other people’s
- 4. Sexual
- Too much tissue surrounding/covering clitoris making access to the clitoris difficult
- Self-conscious with current partner, afraid to get into a new sexual relationship or uncomplimentary comments from a previous partner
- Pain or irritation during sex
- Friction
- Folding of the labia minora into the vagina requiring retrieval
- 5. Psychological
- Negative impact on self-confidence
- Reduced self-esteem with associated insecurity and reluctance to pursue or continue a sexual relationship
There is significant overlap and co-existence between these categories and for any individual woman, any number of these factors may be pertinent.
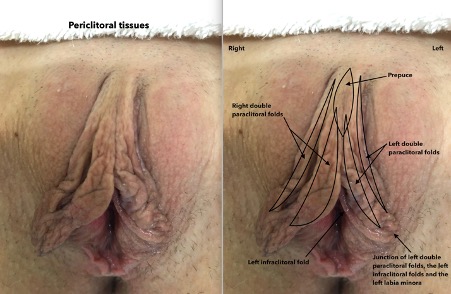
Periclitoraplasty
This describes surgery to the periclitoral tissues. However, the words periclitoraplasty and periclitoral are words created by Dr Oseka Onuma. He made them up to explain the tissues surrounding the clitoris and define surgery to these tissues.
Let’s break up the word Periclitoraplasty and then you’ll understand:
Peri: ‘Peri’ is a prefix which can mean enclosing, surrounding around or near
Clitora: Meaning clitoris
Plasty: Shaping a defect in a body part to restore form or function
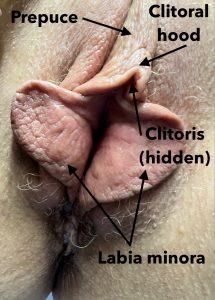
The periclitoral tissues include the:
Clitoral hood: Immediately above the clitoris
Paraclitoral folds: Lateral (to the side of) clitoris
Infraclitoral folds (frenulum): Begin immediately below the clitoris
Prepuce: Found centrally, above the clitoral hood (and in-between any paraclitoral folds)
The upper parts of the labia minora and periclitoral tissues represent the greatest technical challenge with regards to surgery. Nevertheless, the option of periclitoraplasty needs to be considered very carefully because reduction of the labia minora can, in some cases, be achieved successfully only to result in the periclitoral areas appearing more prominent or to continue to obstruct access to the clitoris.
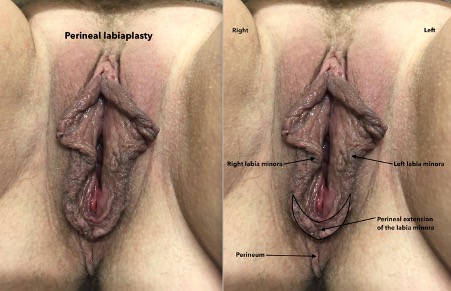
Perineal labiaplasty
This describes surgery to the labial minora where it has crossed into the perineum. The term perineal labiaplasty was created by Dr Oseka Onuma. In addition to refashioning the perineum, this surgery often involves consideration and appropriate reconstruction of the lower parts of the vaginal entrance (forchette and upper perineal body).
Dr Oseka Onuma has gained world recognition for his labiaplasty and labial reconstructive surgeries. His approach involves meticulous attention to tissue handling, dissection, and contouring. He finds labiaplasty surgery to be fascinating and, sometimes, challenging. Achieving consistently good results requires expertise. Expertise does not happen by accident, it requires thought, dedication, and hard work. This is his comfort zone.
For more information simply reach out to us.
For in depth information read my book, ‘So, you want a labiaplasty.’
Excellence in Form and Function. Prevent, Treat and Maintain.
Mons Pubis Reducton Surgery
“The most effective way to reduce the size of the mons pubis in many overweight women is by sensible weight loss. However, this is not universally effective. Isolated enlargement of the mons pubis is not uncommon. In my practice I see many women who have undergone an abdominoplasty resolve abdominal overhang without any reduction of the mons pubis. I am consulted by women who are of normal size and weight but who are bothered by a prominent mons pubis. My technique for mons pubis reduction eliminates the ‘pouch’ and leaves a single scar well below the bikini line.”
A patient’s perspective
‘I’m a woman with one child. I have at times been overweight, and consequently, have excessive fat on my mons pubis. Do you have any ideas about how I would go for having this removed? I had a Tummy tuck and liposuction, because of stretched and loose skin from pregnancy and then weight loss, but it evidently hasn’t worked properly. I am highly embarrassed when it comes to sexual partners and need this to be fixed somehow! I look like I have a “package” as men do when wearing any pants, bathers, etc.’
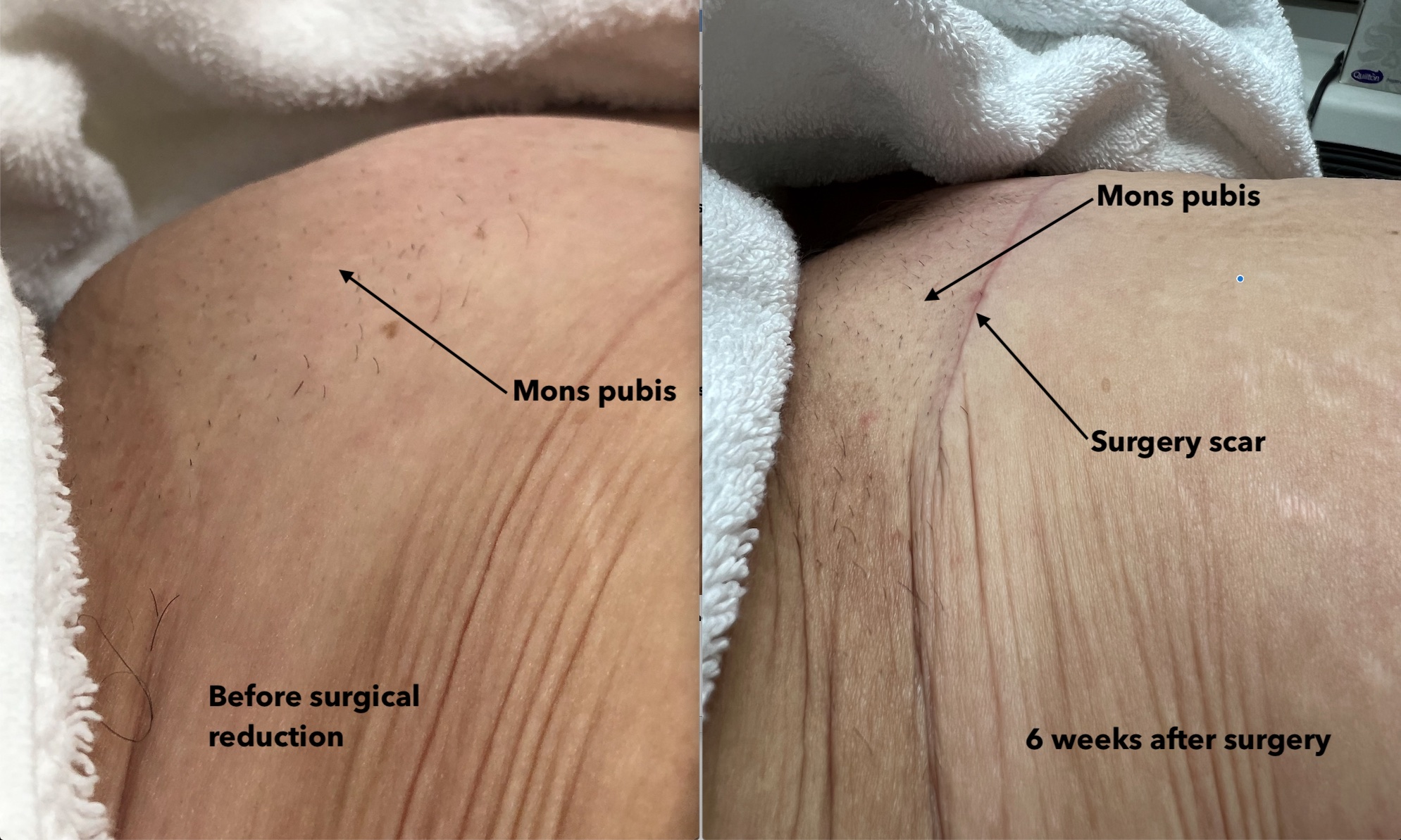
This patient has managed to achieve significant weight loss and then undergone an abdominoplasty. She remained concerned by the weight, prominence and discomfort associated with the mons pubis and labia majora. There had been little or no change in fat deposition in this area and the abdominoplasty had no effect on the enlarged mons pubis. It is important to note that individual outcomes vary and may be affected by numerous factors. It is always important to have a detailed discussion with your surgeon about your own particular circumstances and the potential outcomes and risks associated with any surgical procedure.
What is the mons pubis?
The mons pubis is contiguous with the vulva and, inferiorly, divides into the labia majora. It is a naturally prominent structure that lies in front of the pubic symphysis (the part of the bony pelvis that can be felt at the lowest aspect of the abdomen). The skin is heavily laden with hair follicles and beneath the skin the content is mostly fatty tissue. There are very few nerves within the fatty tissue but there is an abundance of blood vessels.
Prominence of the mons pubis is not exclusive to women with a raised BMI. It also occurs in women considered to be in the normal weight range (for their height), particularly in those who have been previously overweight. Extra fat deposition in these areas can be particularly stubborn to shift even after effective overall weight loss.
Why do women request mons pubis reduction?
Symptoms
- Dragging sensation.
- Feeling of a bulge.
- Impression of carrying a weight, particularly when moving around.
- Irritation when wearing tight clothes.
- Increased, localised sweating.
Aesthetics
- Some women are bothered by the prominence of the mons pubis and how they perceive that it affects their appearance and self-confidence.
Liposuction is not always suitable for mons pubis reduction as removal of fat alone may result in excess loose skin on the surface.
Surgical reduction is the only effective means of reducing the size of the mons pubis.
Direct surgical reduction or debulking of the mons pubis, is in some ways like an abdominoplasty. The incision is very much smaller, and the final scar will be one that is transverse across the mons pubis sited in such a fashion as to be well below the ‘bikini line.’ Nevertheless, there will be a visible scar, which in most cases will gradually fade over time. The principle of this surgical technique is to remove a wedge of excess skin with the underlying fat. Superficially this is done in an elliptical incision with mobilization of the wound edges whilst producing as little disruption to superficial nerves as possible. Women who undergo this procedure may find that they have some minor loss of sensation in the area immediately around the wound although this is much less likely to happen when compared to the more invasive surgery of abdominoplasty which typically produces an area of decreased or absent sensation around the wound.
The operation can be carried out under a general anaesthetic or regional block. Local anaesthesia is always applied to the wound. The length and nature of the incision is determined by the size and shape of the mons pubis. The wound is typically elliptical so that the final wound, when closed, is transverse. A wedge of the fat layer is excised taking care with haemostasis. The amount of fat removed must be judicious to achieve the desired outcome. A pressure dressing is applied to the wound. This reduces the risk of bleeding and bruising in this very vascular area.
Surgery is covered by intravenous antibiotics given during surgery and an oral course of antibiotics to be taken for 5-7 days after surgery. Depending on the time your surgery takes place overnight admission in hospital may or may not be required. You will not be able to drive for 3-4 days post surgery. Return to work should not be less than 7 days and will depend on the nature of your work.
Although more than 90% of healing has taken place by 6 weeks, it will take another 6-10 weeks for the skin wound to completely heal. Healing of the skin wound and reduction in scar formation is encouraged by massaging anti-scar creams/gels or hyaluronic acid serum into your wound. You will receive advice about when to commence this.
Dr Oseka Onuma is an internationally recognized expert in mons pubis reduction. For more information on how he can assist you, please do not hesitate to contact the office.
Book a ConsultationExcellence in Form and Function. Prevent, Treat and Maintain.
Sexual Function Surgery
“Female sexual function is very complex. When there is an abnormality that impacts negatively on the affected woman this is sexual dysfunction and a personal distress component becomes manifested. Physical, hormonal, and psychological factors influence sexual function. Careful exploration, discussion and investigation of your concerns will allow me to tailor surgery and any other treatments to your circumstances.”
A patient’s perspective
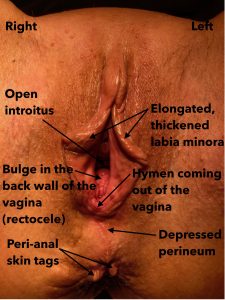
‘Since having my daughter I have lost a lot of sensation during intercourse. At the time of her birth, I had three different people saying to me, “you need stitches,” but I didn’t get any. Now I avoid intercourse because of that reason. It feels like everything is lower, feels like a prolapse, feels like everything is falling downwards. I can see a little lump at the entrance, and I didn’t see that prior to having my daughter. There’s also a skin tear and tag at the entrance where it healed. I saw some doctors, but I was told someone would care for me and love me for who I am. But I’m too embarrassed so how will I meet someone, and then it’s uncomfortable.’
What is sexual function surgery?
Surgery for sexual dysfunction improves sexual dysfunction disorders that have their root in a physically identifiable cause. To achieve this, the principle of surgery is to restore anatomy to as close to normal as possible.
Whilst the resolution of physical problems may result in psychological benefits, surgery is highly unlikely to be beneficial for women whose primary problem has a psychological, psychiatric, hormonal or endocrinological aetiology.
Conditions that may be improved by surgery include some types of:
- Sexual aversion disorder
- Phobic aversion to, and avoidance of, sexual contact with a sexual partner, which must be persistent and causes personal distress. For example, resulting from:
- Urinary incontinence.
- Pelvic organ prolapse.
- Labial discomfort or elongation.
- Vaginal lesions.
- Phobic aversion to, and avoidance of, sexual contact with a sexual partner, which must be persistent and causes personal distress. For example, resulting from:
- Sexual arousal disorder
- Inability to attain/maintain sufficient sexual excitement, causing personal distress. For example, resulting from:
- Vaginal wall relaxation.
- Perineal body detachment.
- Pelvic floor muscle detachment.
- Inability to attain/maintain sufficient sexual excitement, causing personal distress. For example, resulting from:
- Sexual pain disorder
- Dyspareunia – Genital pain associated with sexual intercourse. For example, resulting from:
- Scarred introitus/perineum
- Elongated labia
- Endometriosis
- Uterine and vaginal wall prolapse
- Vaginal dryness
- Dyspareunia – Genital pain associated with sexual intercourse. For example, resulting from:
- Vaginismus – Involuntary spasm of the musculature of the outer third of the vagina that interferes with vaginal penetration, which causes personal distress.
Dr Oseka Onuma has a particular interest and expertise in female sexual function disorders that have a physical basis in the pelvic area. He regularly performs surgery and treatments to alleviate the conditions that have resulted in sexual dysfunction. Dr Onuma is highly trained and experienced in both surgical and non-surgical techniques aimed at raddressing the physical factors associated with female sexual function disorders.
For more information on any of the conditions noted above that have affected your ability to be sexually active, please do not hesitate to contact the office.
Book a ConsultationExcellence in Form and Function. Prevent, Treat and Maintain.
"The Ultimate V" - Concept, Thesis & Application
“I want you to, for a moment, close your eyes. Imagine that you are about to begin a journey somewhere way out of your comfort zone. Now, begin to see that journey with a guide who knows the route, the diversions, the potential traps, and pitfalls, who understands your fears and your desires. A guide who could place the very words that you are thinking in your mouth just as you struggle to get them out. That guide is me, Oseka Onuma, and I plan to hold your hand and steady your course on this, your personal journey.
My concept of “The Ultimate V” began many years ago when I received the 2 emails below:
‘Dear Dr Onuma
Firstly, I would like to thank you for providing such an excellent and informative website for your viewers. I have found much comfort in knowing that I am not alone, and that many women share the same problem that I have. Thank you for bringing this issue out in the open, because I have been through a period of anger and depression, and even resentment towards health professionals for not providing any information on the topic of female sexual gratification and for not informing women that problems like this can be corrected.
I am sad that so many women, including myself, have suffered in silence or accepted it as normal, at the expense of enjoying a fulfilling sex life once again.
I have two children, both, delivered vaginally. With my first child, six years ago, I was advised by friends to avoid a caesarean section at all costs, since it would weaken my abdominal muscles and I would never achieve a flat stomach again. So, I asked my midwife to let me push for as long as I could, and that a caesarean section should be the very last option. My labour lasted 15 hours, and I pushed for a good hour but got into difficulty as the baby was not descending. I went to theatre and baby was delivered by ventouse; with or without episiotomy, I am still not sure. My midwife told me I tore, but my delivery record says I had episiotomy. I had six stitches.
I never regained the vaginal tone, or pelvic floor strength that I had before, despite doing regular pelvic floor exercises. I immediately noticed a change in the appearance and the size of the vaginal opening, and this has really distressed me since. Most disturbingly, my enjoyment of sex has greatly diminished because of the lack of tone in my vaginal muscles. Of course, after having my second child nine months ago, my situation got worse. I am so disturbed by the appearance of my vagina that I don’t like my partner to look at me. Sex is even less fulfilling than before, and the whole situation has started to affect my self-esteem. I used to enjoy a very active sex life with my partner, but now, because I don’t enjoy sex as much, I don’t want sex as much. I feel very unattractive and unfeminine.
After having my second child I actually thought that what I was seeing was a bladder and/or bowel prolapse and became very depressed about it. I found it impossible to share my feelings with my partner, so I found a very good GP and we both went along to see her together. She examined me and told me that I do not have a bladder/bowel prolapse, but a minor prolapse of the vaginal wall. She said it was normal for someone who has had two children, and that I should try pelvic wall exercises religiously for three months. If after that, I found no improvement and was still distressed, she would refer me to a gynaecologist.
As I mentioned earlier, I went through a period of resentment towards the health profession, especially for not fully informing women of the trauma following childbirth and for not providing more options for the type of delivery to have. Whilst I have achieved only minimal improvement with pelvic floor exercises, I have yet to go back to my GP for referral to a gynaecologist. Partly, because I think a major source of my frustration was that I could not share this with my partner, but we have since worked through it and he is very supportive. Also, I am frightened that the gynae will not be as understanding as my GP and give me more exercises to do. I’m sure you have heard this from other women Dr Onuma, but I have very little faith in these exercises to restore my body to even a fraction of what it was before.
My GP told me about a doctor here that does “Designer Vaginas”, but I just laughed it off. I really didn’t think that real women had that sort of surgery, that it was only reserved for the rich or the weird. I actually didn’t know that it really existed, until a friend of mine told me that her sister had it done. So here I am, seriously considering having this procedure done myself. I want to feel attractive and feminine again, and to achieve a fulfilling sex life with my partner like before. Without those things I don’t even feel like me anymore, it really has affected my self-image. So, I am asking for your help Dr Onuma. Once again, thank you so much for doing what you do, and for making what is such a sensitive topic easier to talk about.’
‘When I initially looked for a gynaecologist to help me with my concerns; when I told them, “Not only am I concerned about my rectocele, but my labia majora are sagging, my labia minora are too long and my vagina is quite loose.” Their focus was on just repairing my rectocele and that was the end of it.
When I mentioned my other concerns, the look on their face made me feel rather foolish. It was already an embarrassing problem, and it became even more embarrassing when I was made to feel silly. I actually had a doctor say to me, “Oh, you’ve just had two kids. You should see women who have had four kids, it’s like you can drive a bus in.” So basically, it was like, “Be happy you didn’t have two more kids.” Basically, you are left with the impression that it is something you just have to live with.’
“The Ultimate V” is a personalised, tailored programme, transitioning from Concept & Thesis, through to application. It has been created by me, for you. It is unapologetic in its aim, to restore your pelvic floor function. Individual outcomes reflect the wide variety of concerns and circumstances which exist and as such, every patient is treated as an individual and counselled about potential outcomes, risks and recovery. I will treat and, with my assistance, you will maintain.”

“The Ultimate V” – Concept, Thesis & Application
Surgery
- Labiaplasty
- Vaginoplasty
- Hymenoplasty
- Mons pubis reduction
- Sexual function surgery
Treatments
- Laser treatments
- Platelet Rich Plasma (PRP) treatments
- Radiofrequency needling
- Healite LED therapy
Dr Oseka Onuma believes that expertise does not happen by accident, it requires thought, dedication, and hard work. This is his comfort zone. However, expertise is not enough. Empathy combined with experience set him apart from the conventional approach to pelvic floor medicine and surgery. When you are ready, he will be here for you.
For more information simply reach out.
For in-depth information read my book, “The Ultimate V”.
Excellence in Form and Function. Prevent, Treat and Maintain.
Vaginoplasty Surgery
“Vaginoplasty surgery for women is about reshaping and reconstructing the vagina and the structures that compose the entrance to the vagina (the ‘introitus’) in an attempt to restore normal anatomy. Vaginoplasty has both functional and cosmetic components which are intricately linked. Although confusion about terminology is common for the female pelvic floor, I would stress that vaginoplasty does not involve surgery to any structures beyond the entrance of the vagina.
My book, ‘Vaginoplasty‘ addresses the current scarcity of detailed information for women considering vaginoplasty. I believe that it is essential reading for women considering surgery.”
What is vaginoplasty?
Vaginoplasty is a blanket term used to describe any surgery to change the shape or function of the vaginal canal, the entrance, the supporting structures at the entrance and at the top.
This includes:
- Vaginal tightening surgery
- Vaginal loosening surgery (levator muscle and scar tissue division)
- Perineal body reconstruction (vaginal entrance tightening)
- Fenton’s plastic repair (vaginal entrance loosening)
- Vaginal wall lesions and skin tags
- Hymenoplasty (reconstruction and reduction)
- Prolapse surgery
- Posterior vaginal repair
- Anterior vaginal repair
- Uterine suspension
Vaginoplasty to improve sensation during intercourse is reserved specifically for those women who complain that because of reduced vaginal sensation (due to vaginal wall relaxation/prolapse) their enjoyment of sexual intercourse has been diminished. It can also be of significant value in women who, because of vaginal wall scarring (e.g., result of tears or episiotomy during childbirth or previous vaginal surgery) suffer from pain during intercourse or an overtight vagina where intromission has become painful or impossible.
A patient’s perspective
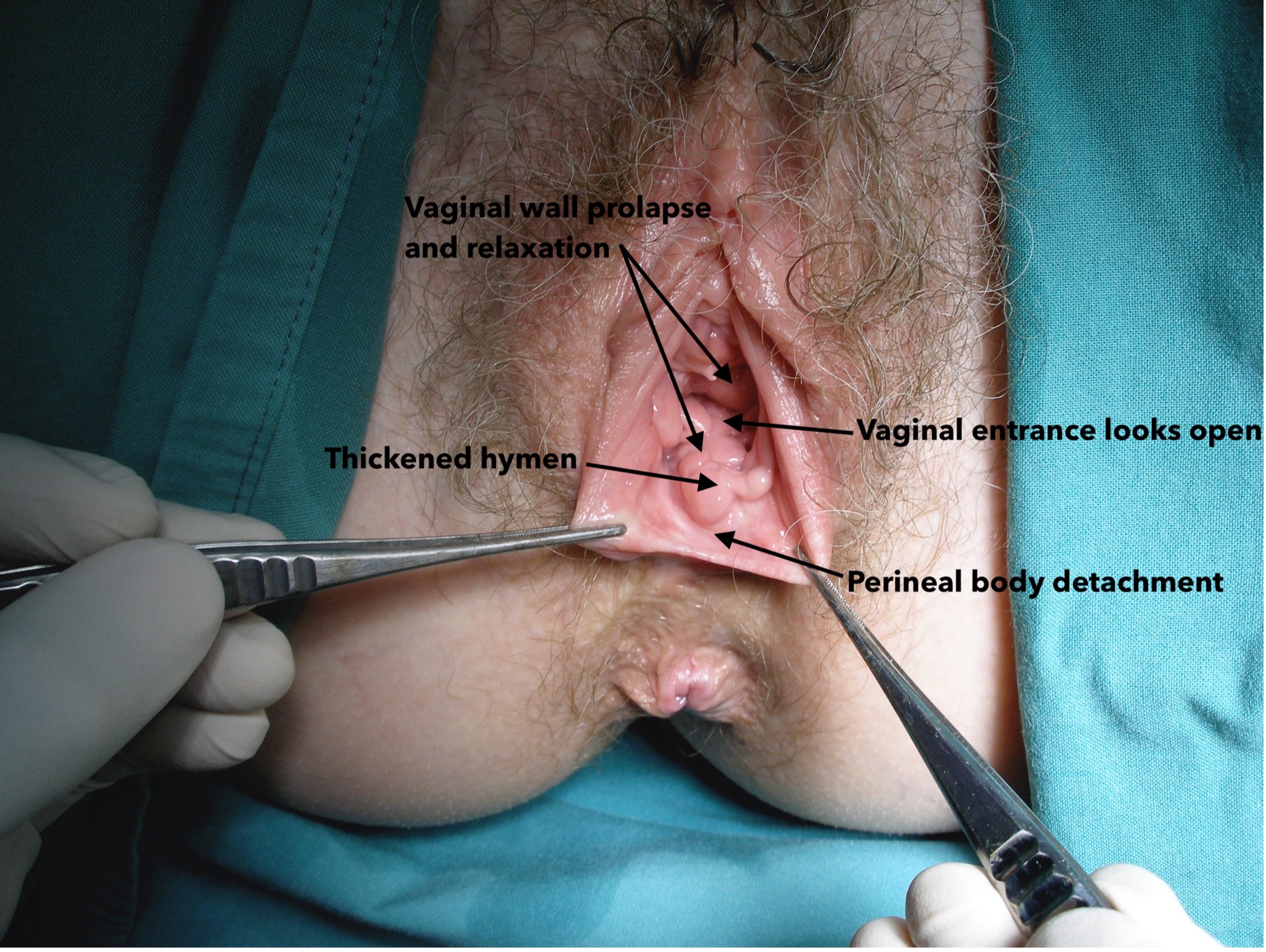
The patient below complained of reduced sensation during intercourse, the impression of a bulge within the vagina and the impression that the vagina was much more patulous than it had been before having children. She reported being embarrassed by the occurrence of vaginal flatus, faecal trapping, much reduced ability to achieve orgasm through vaginal stimulation and felt disconnected during intercourse because of reduced lack of sensation. On examination I noted a grade 2 prolapse of the front and back walls of the vagina, relaxation of the vaginal walls and thickening of parts of the hymen. The interior diameters of the vagina were capacious. She had grade 2 uterine descent and evidence of perineal body detachment.
Dr Oseka Onuma has a particular interest and expertise in vaginoplasty surgeries. He is highly trained and experienced in all aspects of vaginoplasty aimed at restoring pelvic function with a focus on femininity. Patients who have already undergone gender re-assignment surgery may have confidence when seeking to improve the external appearance under his care.
For more information on any of the conditions noted above that have affected your ability to be sexually active, please do not hesitate to contact the office.
Book a ConsultationExcellence in Form and Function. Prevent, Treat and Maintain.
Clitoral Surgery
“The clitoris is a long, complicate organ with a dense nerve and blood supply. It is a very important part of the genital anatomy and responsible for much of the sexual satisfaction and pleasure experienced by women.
For some women the clitoris is too prominent or exposed resulting in increased friction (due to rubbing against undergarments and clothes) leading to discomfort and hypersensitivity or aesthetic concerns due to the size and prominence. Both concerns often co-exist in women who complain of clitoral enlargement.
Clitoral enlargement (clitoromegaly) can be present at birth or develop later in life. Most often, exposure to androgens (mainly testosterone) causes this to occur in people designated female at birth. It is normal for the clitoris to increase in size during arousal but this increase will reverse when arousal has stopped. In true clitoromegaly, the visible part of the clitoris (the ‘glans’) remains larger than the typical ¾ to 1 inch. Other causes of clitoral enlargement include cysts, noncancerous tumours or irritation to the external genitals (vulvitis), congenital conditions (present at birth) and hormonal changes in polycystic ovarian syndrome and increased androgen levels (particularly testosterone) in the blood stream.
Clitoral surgery has both functional and cosmetic components which are intricately linked. Clitoral surgery is very specialised surgery involving specific techniques and skill which I have travelled internationally to acquire.
Dr Onuma is the author of ‘So, You Want A Labiaplasty‘ and ‘The Ultimate V‘. These books are unique and aimed at women considering their options for labial, vaginal and pelvic floor improvement.
Common causes of an enlarged clitoris in children:
Congenital adrenal hyperplasia is a congenital condition (disorders present at birth) in which persons designated female at birth may have such an enlarged clitoris that it may resemble a small penis. This is due to exposure to too many androgens during fetal development. Androgens are sex hormones associated with being designated male at birth.
Causes of an enlarged clitoris developing in adulthood:
Hormonal changes that can lead to clitoromegaly are usually consequent to increased levels of androgen. Conditions that may cause this include:
- Polycystic ovarian syndrome.
- Adrenal gland tumours.
- Use of anabolic steroids.
- Testosterone replacement therapy.
Before and after clitoral reduction without labial surgery:


The technique used for clitoropexy in this case has also reduced the protuberance of the labia minora without needing to proceed to labia minora reduction. This is an individual case and are not reflective of all outcomes. A detailed discussion is required to prepare you for potential outcomes, risks and recovery from surgery.
The recovery period for clitoral surgery depends on the patient and whether concomitant clitoral hood surgery or labiaplasty is undertaken. In general, patients can expect the same experience as they would for a labiaplasty including discomfort, swelling, and bruising but this will mainly involve periclitoral tissues. The symptoms associated with a clitoral hood surgery are often managed with pain medication and occasionally, ice packs.
Surgery to reduce the clitoral hood and prepuce is much more commonly requested and indicated surgery than clitoral reduction simply because excessive paraclitoral tissue is more common than clitoromegaly.
An example of redundancy and excess of the prepuce and clitoral hood resulting in a hidden clitoris is shown below.
For more information on any of the conditions noted above, please do not hesitate to contact the office.
Book a ConsultationNon-Surgical Treatments
Bladder Problems
Unless we have a problem with our bladder function we remain largely unaware of the multiple, complex, interacting systems that work to maintain subconscious control and allow effortless voluntary oversight. We are not born with these systems working effectively. During early childhood the appropriate neural networks become established and increasing conscious brain control allows the transition from functioning as a baby to developing control over when and where to empty the bladder.
It should come as no surprise that many women who seek help for their bladder problems, incontinence especially, do so because of a fear of returning to this childhood state as they get older. This fear may be exacerbated by an experience of either seeing their mother or another female relative devolve into a situation of incontinence with its’ myriad social and hygienic sequelae or had personally suffered an accident in public circumstances.
In order to appreciate what might constitute a bladder problem, we need to have a basic idea about that the bladder should do:
- A residual urine volume of less than 50ml.
- The first desire to void occurs when there is between 150-200ml of urine in the bladder.
- A bladder capacity between 400-600ml.
- No rise in bladder pressure during bladder filling or when standing.
- There are no unprovoked spasms of the detrusor muscle of the bladder.
- No leakage of urine during activities such as coughing, sneezing and laughing.
- The amount of urine voided should be at least 150ml.
- The peak flow rate during voiding should be greater than 15ml/sec.
You should not have to constantly worry about having a bladder accident. During the day emptying should not take place more than 7-8 times and no more than 1-2 times (age dependent) at night. If you feel the need to empty your bladder, you should be able to wait without fear of having an accident. When you do emptying your bladder, the urine should not trickle out, with you sitting on the toilet for what seems like ages. You should not have to do any specific manoeuvres (such as sitting forwards or straining) in order to empty your bladder.
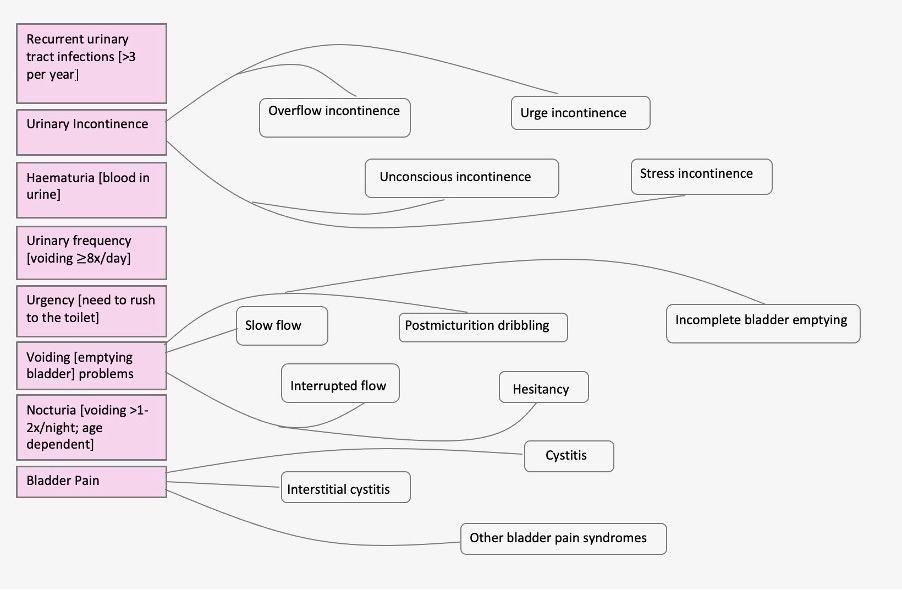
What are bladder problems?
Bladder problems (dysfunction) is a collective term for abnormalities of how urine enters the bladder (filling), is stored and emptied.
Dr Onuma’s approach to bladder problems
The bladder is a liar. When is misbehaves it does odd things making it difficult for the person suffering the symptoms to actually explain what they think is going on. The problems produced by different conditions often overlap and different conditions may affect the same individual. Some of those conditions may require a treatment which may not benefit another existing bladder condition.
Dr Onuma takes a very systematic approach involving:
- History.
- Examination.
- Investigations.
- Treatment.
- Treatment response assessment.
- Modification of treatment as required.
Non-surgical treatment options are tailored to the specific problems and circumstances of the individual patient and may include:
- Conservative therapies
- Lifestyle modifications
- Pelvic floor muscle training
- Biofeedback
- Bladder training
- Rejuvenation medicine therapies
- Platelet Rich Plasma (PRP) treatment
- Laser vaginal treatment
- Oral medications
- Anticholinergics
- ß-adrenoceptor agonists
- Tricyclic antidepressants
- Antibiotics
- Intravesical medications (solutions placed in the bladder through the urethra)
- Heparin
- DMSO
- Oxybutynin
- Nerve stimulation
- Percutaneous tibial nerve stimulation
- Sacroneuromodulation
- Acupuncture
- Magnetic chair
Dr Oseka Onuma has a particular interest and expertise in female bladder problems using non-surgical and surgery to restore continence, alleviate pain and prevent recurring bladder infections. He is highly trained and experienced treating lower urinary tract problems in women and is on the Expert Witness register of the Australian and New Zealand College of Obstetricians and Gynaecologists for urogynaecology.
For more information on any of the conditions noted above or about surgical solutions for urinary incontinence, please contact the office.
Book a ConsultationExcellence in Form and Function. Prevent, Treat and Maintain.
Depigmentation
“Intimate hyperpigmentation is a disorder caused by an excess formation of melanin that involves skin darkening around the vulva, inner thighs and groins. This is more noticeable for women who have removed the hair in the genital area, and some will be bothered by an impression of a ‘stained skin’ effect. The trend towards hair removal has influenced the demand for depigmentation treatments. In Australia, depigmentation products are heavily regulated to prevent the use of toxic products which are harmful to health.
The process that leads to hyperpigmentation is dynamic and ongoing. It can be accelerated in certain conditions such as pregnancy due to hormonal changes. The genital area is not the only body part affected as changes can also be seen in the nipple, areola of the nipple and underarms. Surgical and non-surgical treatments for hyperpigmentation may have a role to play depending on the site(s) affected. Non-surgical maintenance therapies should not be ignored if recurrence is to be prevented.”
The parts of the vulva that can be affected by hyperpigmentation include
- Mons pubis
- Labia majora
- Labia minora
- Vaginal opening (introitus)
- Perineum
- Peri-anal tissues

Depigmentation treatments available with Dr Onuma
Surgery:
- Vaginoplasty
- Perineal body + perineum reconstruction
- Labial reduction
- Labiaplasty (minora/majora)
- Periclitoraplasty
- Scar excision
- Mons pubis reduction
Non-surgical:
- Fractional laser skin treatments
- Hormone management therapies
- Platelet Rich Plasma (PRP) treatment
- Medications
Surgical management of the hyperpigmented vulva by Dr Onuma
Before

After

Why does the vulva get darker?
Hyperpigmentation is caused by numerous factors. The main trigger factors include:
- Age
- Normal ageing of the vulval tissues results in changes in biological, biochemical, and molecular mechanisms which can lead to pigmentation disorders
- Genetic predisposition
- Persons with darker skin (phototypes IV, V and VI) are more likely to be affected
- Hormonal changes
- Oestrogen stimulates the activity of tyrosine, the enzyme responsible for melanin production
- Care and beauty habits
- Removal of hair can lead to abrasion and folliculitis leading to skin inflammation which stimulates the production of melanocytes, and therefore, of melanin
- Clothing habits
- Friction on the skin leads to skin thickening and the appearance of darker areas. The current trend towards wearing tight pants or underwear has led to an increase in incidence of this outcome
Melanin is responsible for pigmentation. How is it produced?
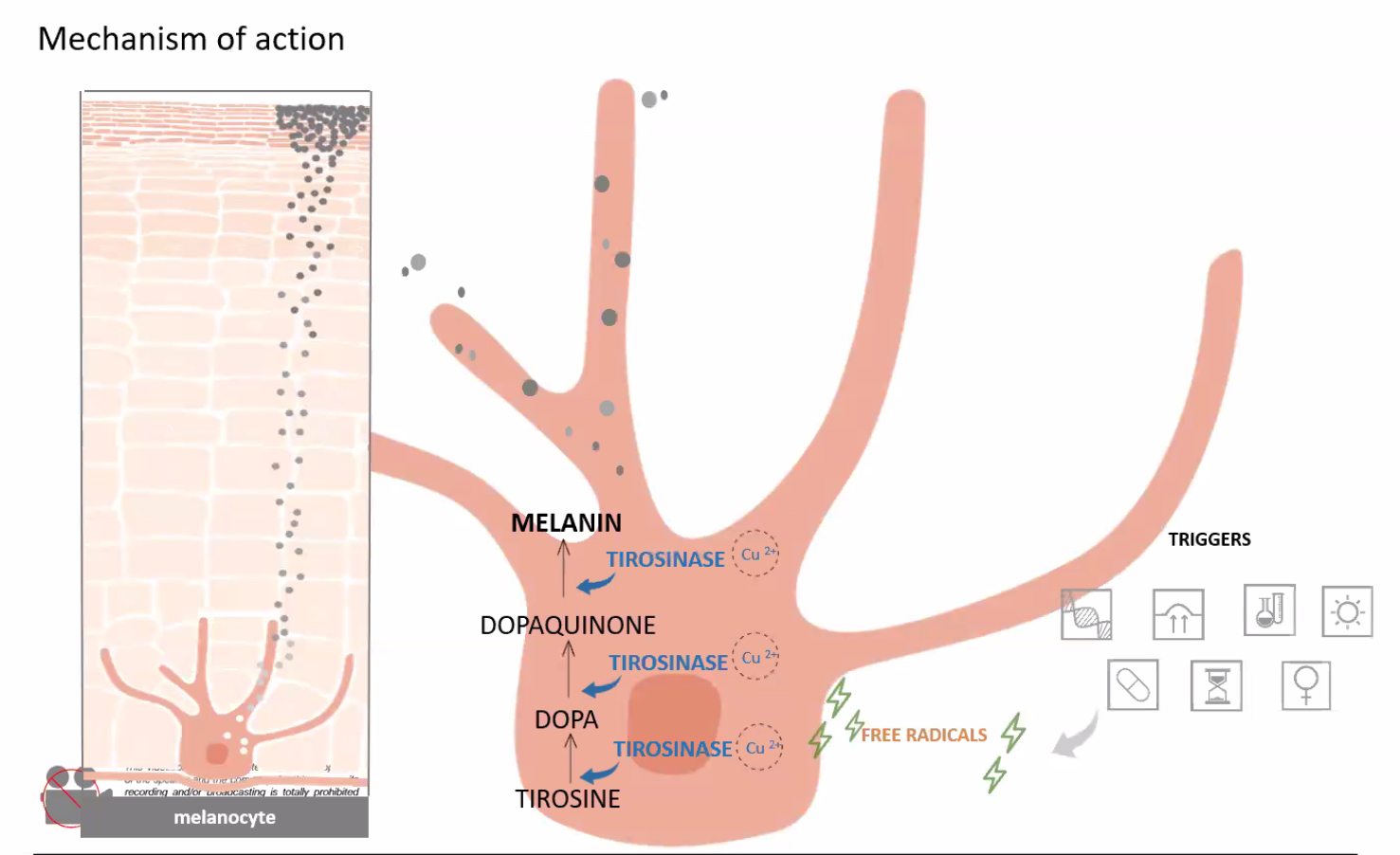
Any product that reduces the process of hyperpigmentation must interrupt part of the pathway involved in the production of melanin.
Dr Oseka Onuma will customize the treatments you need based on your personal circumstances and requirements.
For more information on any of the conditions noted above or about surgical solutions for urinary incontinence, please contact the office.
Book a ConsultationExcellence in Form and Function. Prevent, Treat and Maintain.
Healite II LED Phototherapy Treatment
Dr Onuma uses the Healite for:
- Improving healing times
- Relieving pain
- Subsiding active acne
- Promoting skin rejuvenation
Features of the Healite system:
- LEDs are semiconductors that convert electrical energy directly to light
- Ideal wavelength
- Powerful enough to penetrate deep where it is needed
- Works at subcellular, cellular and tissue level
- Works alone or as an adjunctive therapy
- Treats multiple indications
- Pain-free, non-invasive, treatment of patients all ages
This is an office, non-surgical treatment. Current research indicates that the risk of adverse events is extremely low when performed by well trained, experienced operators.
Treatments
- Wound Healing
- Pain Relief
- Infrared light source can be used to provide temporary relief of muscle and joint pain
- Arthritis
- Muscle Spasm
- Infrared light source can be used to improve local blood circulation
- Reduction of vulval epithelial relaxation
- Skin Rejuvenation
- Reducing fine lines and wrinkles
- Active Acne
- Superficial skin lesions
What Healite II is proven to do:
- Encourages wound and cellular healing post-laser or post-surgery
- Reduces pain, Swelling and redness
- Increases blood flow to the wound
- Decreases the risk of bruising
- Decreases recovery time
- Offers prophylaxis against scar formation
- Reduces PIH (post inflammatory hyperpigmentation)
- Improves the clinical results
Excellence in Form and Function. Prevent, Treat and Maintain.
Infini Radiofrequency Treatment
Infini RF treatment is a non-surgical office procedure. It is a long-term tissue rebuilding treatment. The clinical results should be long lasting like a fractional laser treatment (up to 3 years depending on the health of the skin and how the skin is looked after). Although some patients see results very quickly, most will recognise improvements 3-4 weeks after the first treatment. Optimal results are seen 3-6 months after the final session due to new collagen development.
The Infini RF
- Can be used in all skin types including tanned skin.
- Minimal risk of hyperpigmentation.
- Can treat scars of all types.
- Very few limitations as to where the skin can be treated on the body.
- Active inflammatory acne
- Acne scars
- Hyperhydrosis (excessive sweating)
- Excessive sebum secretion
RF in the practice of medicine:
- High frequency radiofrequency has been used in the practice of medicine for over 70 years.
- 2002: The first device cleared by the FDA for dermatological procedures for electrocoagulation.
- 2009: Cleared by the FDA for non-invasive treatment of wrinkles and creases.
Definition of ‘Skin Tightening’:
- The FDA does not recognise ‘skin tightening’ as an indication because this term is difficult to define.
- ‘Skin tightening’ really means a reduction in the appearance of lax skin. It does not necessarily mean that the skin shrinks or becomes stiffer.
RF for tightening the skin:
- How does it work?
- Heating the dermis to a high enough temperature causes collagen coagulation.
-
- Collagen coagulation results in immediate skin shrinkage and initiates the wound healing process.
- New collagen and elastin formation takes place.
- New collagen replaces old collagen during remodelling.
- The higher the temperature:
- the more RF energy is required.
- this produces more visible results.
- the more intense the degree of coagulation and the shorter the required exposure time to heat required.
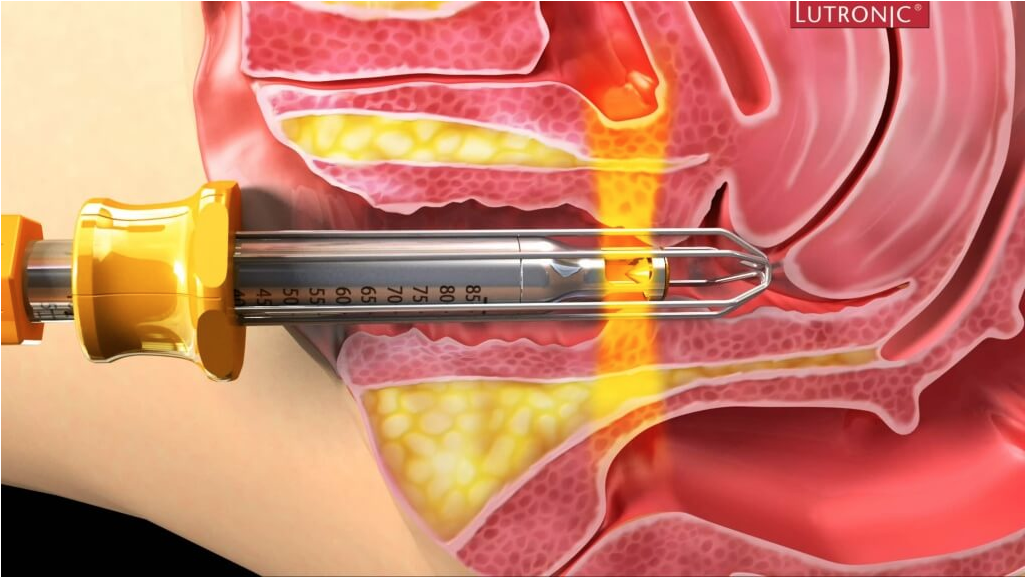
The Infini RF system – why combine RF with needles?
The benefit of micro needling is that the trauma from the needles penetrating the skin causes mechanical stimulation to fibroblast cells in the skin to also help in producing collagen
- Uses an array of ultrasharp needles (200 microns in diameter).
- Variable depths of skin penetration from 0.5mm to 3.5mm in 0.5mm increments.
- Allows predictable treatment of several levels of the dermis.
- The use of shallower depths is particularly important in thin areas of the face such as the areas below the eyes.
- In most (but not all) parts of the body treated with Infini RF, 3 passes are made.
- The first pass is set to deliver energy at the deepest level and the final pass at the shallowest level.
- At each activation the needles enter the skin, deliver the RF energy and withdraw, leaving a discrete zone of thermal damage at the pre-set depth.
The approximate treatment time is between 20-30 minutes; however, a local anaesthetic ointment needs to be applied for 45-60 minutes prior to commencing treatment. The recommended number of sessions is 3. The minimum interval between sessions is 4 weeks. Repeat treatments may be beneficial every 6-12 months depending on the indication for treatment and whether other treatments are being applied at the same time.
Preparation for treatment
7 days prior to treatment
- Stop taking supplements that increase bleeding/bruising such as:
- green tea, fish oils, Evening Primrose oil, garlic, Echinacea, St John’s wort, Vitamin E, Non-steroidal drugs and aspirin (*only after discussing with your doctor)
- Before attending for treatment, you can use some simple analgesia such as paracetamol but not any non-steroidal anti-inflammatory drugs such as Nurofen or Ibuprofen (which interfere with platelet function).
- It is best to be well hydrated, so drink plenty of water in the 4-5 hours prior to treatment.
- After treatment, continue to drink water liberally and use simple analgesia (not non-steroidal anti-inflammatory drugs) if required.
Post treatment care instructions
- Avoid hot showers or saunas on the day of treatment.
- Gentle washing with warm or cold water only.
- You may feel a burning sensation for 1-2 hours after treatment and the feeling of heat on the treated areas for several more hours. You can apply;
- a wrapped ice pack or frozen gel pack but avoid direct contact with the skin.
- Pinpoint bleeding is a normal skin reaction on the day of treatment;
- Dab the area with clean cotton pads.
- Avoid using makeup for 24hrs. If essential a mineral make up can be applied.
- Rarely, the skin tone can become darker with crust formation from 1-2 days after treatment;
- This is a normal process and will resolve by itself.
- Do not forcibly scrub or remove epidermal debris;
- Please leave them to exfoliate naturally.
- Never use scrubbing agents or exfoliants.
- Avoid using alcohol-based cosmetics for at least 2 weeks after treatment.
- Use moisturising agents frequently.
- Apply a UV-A/B sunblock with SPF of 30+ regularly and use physical sun protection (ie. hat/umbrella) when outdoors to reduce the risk of hyperpigmentation.
- Avoid vigorous activity, alcohol consumption, exercise and sauna for at least 7 days post treatment.
- Do not use retinoids (Fit A containing preparations) for at least 1 week before or after treatment.
Skin reaction after treatment
- Immediately post treatment:
- Redness and transient oedema.
- Resolves spontaneously after 1-2 days.
- 1 day post treatment:
- Redness and oedema begin to resolve.
- Skin returns to a condition similar to before the treatment.
- 3-7 days post treatment:
- Brighter skin tone.
- Reduction in sebum secretion in oily skin types.
- 1 month post treatment:
- Improvement in appearance of fine wrinkles and skin laxity.
- 1-3 months post treatment:
- Continuous improvement in the appearance of fine wrinkles, pores, scar and skin laxity.
Contraindications to treatment with the Infini RF system
Absolute contraindications
- Tendency to keloid formation
- Allergy to local anaesthetics, some antibiotics, or medications
- Haemorrhagic disease
- Photo-sensitive skin
- Diabetes
- Acute inflammatory skin disease (other than inflammatory acne)
- Patient with a cardiac pacemaker, defibrillator, or cochlear implant
- Patient unwilling to accept risks
Relative contraindications
- Acute or chronic infection
- Some metabolic disorders
- Current significant drug or alcohol abuse
- Some mental health problems
- Some chronic skin diseases
- Some systemic disorders
- Skin lesions resulting from diabetes mellitus, connective tissue disorders, radiation therapy or chemotherapy
Risks of Radiofrequency treatment
Temporary:
- Bruising
- Oedema
- Pinpoint bleeding on the skin
- Pain
- Skin crusting
- Sensation of skin heat or burning
Potentially significant and not always temporary
- Infection
- Acne flare up or herpes simplex activation
- Rarely:
- Superficial skin burn
- Hyperpigmentation
- Rarely – burn
Outcome
- Whenever any treatment is applied there is the possibility that the recipient may not be happy with the outcome of the treatment.
- More than one treatment in the initial course is required to achieve the desired results.
- A discussion about options for further or other treatments should take place with your doctor.
Excellence in Form and Function. Prevent, Treat and Maintain.
Laser Vaginal Treatment
A laser device produces an intense, narrow beam of light (or other radiation). Lasers have broad applications, being used in engineering, the music industry and medicine.
Dr Onuma uses the Petit Lady Action II which has the following features:
- A solid-state laser
- Erbium YAG (Er:YAG)
- Wavelength – 2.9 micrometre
- Commonly used in skin resurfacing
- Non-ablative
- Allows controlled heating without burning vaginal epithelium
- Promotes Collagen fibre shrinkage and remodelling
The Action II is a 2940 nm Er:YAG laser system, with excellent absorption in water: as the vaginal mucosa has a high water content, this makes it an ideal and safe target for this laser wavelength. Collagen remodelling of the vaginal mucosa tissue is encouraged by the photothermal effect of the laser, which promotes thickening of the walls of the vaginal canal through collagen regeneration.
- The Action II Petit Lady has a 90° hand piece that directs the laser at a right angle for treatment of the suburethral tissues, thereby improving support. It can also be used to treat the forchette and the junction of the labia minora and introitus.
- A fractional hand piece is used for treatment of the labia minora, labia majora, mons pubis and scars such as those from a Caesarean section.
- A 360° hand piece directs the laser beam circumferentially through the vaginal wall epithelium.
Laser vaginal treatment involves the application of a laser to treat the vaginal walls, introital area or vulva. It is a non-surgical, office treatment.
Treatments
The approximate treatment time per area is 15 minutes. The recommended number of sessions is 3. The interval between sessions is 1-2 weeks. Repeat treatments may be beneficial every 4-6 months in some cases. Normal activities of daily living can be resumed immediately. Sexual intercourse should be deferred for 1-2 days.
- Reduction of vaginal wall atrophy
- A set of aggravating symptoms related to vaginal atrophy generally become worse over a period of time. Symptoms are vaginal dryness, burning sensation, vaginal discharge, genital itching, burning with urination, and reduced vaginal lubrication during sexual activity. For those who suffer from vaginal atrophy, their decreased oestrogen levels cause thinning, drying and inflammation of the vaginal wall. One myth about vaginal atrophy is that the condition happens most frequently after the menopause, but it can actually occur during breast-feeding or at any time when the oestrogen levels drop
- Vaginal tightening
- Sexual gratification may be significantly influenced by the degree of vaginal tightness in some women. Vaginal Rejuvenation aims to make the vestibule and vaginal canal narrower and, thus, increase the amount of friction produced during intercourse. This may improve sensation and enhance sexual satisfaction
- Vulval tightening and resurfacing
- Mons pubis tightening and resurfacing
- Sexual gratification improvement
- Reduction of vulval epithelial relaxation
- Reduction &/or improvement of the appearance and texture of scars
- Improves the appearance of pigmented vulva
- The fractionated laser setting can help restore the natural colour and texture of the vulva by improving collagen formation, tightening the skin and reducing hyperpigmentation
- Mild stress urinary incontinence
- Stress Urinary Incontinence (SUI) is defined as unintentional or uncontrollable leakage of urine due to the weakened tissues supporting the urethra. The tissues supporting the pelvic floor and the urethra (in particular the suburethral area and the bladder base) may be strengthened by laser treatment
- Non-surgical laser treatment is highly unlikely to cure moderate or severe stress urinary incontinence
- Overcome some post-delivery vaginal wall changes
- Pregnancy, labour, and vaginal delivery are significant events in the development of symptoms of decreased sensation and deterioration in vaginal tissues. All three events negatively impact the tightness, tone, control, and strength of the vagina. Non-surgical laser vaginal treatments can restore tightness and elasticity of the vagina
Excellence in Form and Function. Prevent, Treat and Maintain.
Platelet Rich Plasma (PRP) Treatment
- This is an office, non-surgical treatment. Current research indicates that the risk of adverse events is extremely low when performed by well trained, experienced operators.
- The use of your own blood means that there is no risk of transmitting infection.
What is a Platelet Rich Plasma?
- PRP is defined as an autologous (tissues or cells obtained from the same individual) concentration of platelets in plasma with a greater concentration than in whole blood.
- The term ‘PRP’ is used to describe blood Plasma with a high concentration of platelets.
- Platelet Rich Plasma (PRP) is one of a number of modalities of treatment in the field of regenerative or rejuvenative medicine where it is used to aid the body to heal itself.
- The Plasma contains platelets, platelet-derived growth factors and other bio-stimulating factors that play a key role in the body’s natural wound-healing response.
- PRP is activated through contact with extracellular matrix.
- The activated growth factors induce new cellular tissue regeneration including new collagen, new blood vessel formation and nerve growth.
- PRP also has antioxidant effects.

PRP for gynaecology and cosmetic gynaecology
Vaginal walls and introitus
- Promotes Collagen fibre shrinkage and remodelling
- Reduction of vaginal wall atrophy
- Reduction in atrophy of vaginal entrance
- Reduction of vaginal wall relaxation
- Vaginal tightening
- Sexual gratification improvement
- Reduction of painful intercourse
- Reduction &/or improvement of the appearance and texture of scars
Clitoris
- Promotes Collagen fibre formation and remodelling
- Small increase in size of clitoris
- Increase in clitoral sensation
Lichen sclerosus
- Improves the treatment of lichen sclerosus
PRP for cosmetic medicine
- Promotes Collagen fibre shrinkage and remodelling
- Improvement of appearance of the skin surface
- More youthful appearance
- Reduction of fine lines
- Reduction in laxity of jawline
- Mild reduction in sun damage and pigmentation
- Reduction &/or improvement of the appearance and texture of scars
- Reduction of symptoms directly associated with a scar
- Emerging new treatment for androgenic alopecia
- Increase in number and density of hair cells noted
- May improve outcomes of hair transplantation
What does PRP treatment involve?
Draw blood
- Blood is obtained from the best accessible part of the arms, usually in front of elbow. Sometimes the blood may need to be taken from the wrist or back of the hands.
Separate the blood elements
- The specialised tubes are placed into a dedicated centrifuge and spun at several thousand revolutions per minute. This separates the components of the whole blood.
Remove the plasma
- Plasma is removed from the tube leaving behind the red blood cells.
Contraindications to PRP treatment
- Absolute contraindications
- Current use of blood thinners
- Heavy smoking
- Current significant drug or alcohol abuse
- Critically low platelet levels
- Patient unwilling to accept risks
- Relative contraindications
- Acute or chronic infection
- Some metabolic disorders
- Uncontrolled thyroid dysfunction
- Chronic liver disease
- Some chronic skin diseases
- Some systemic disorders
- Low platelet count
- Platelet dysfunction syndrome
- Low blood fibrin levels
Excellence in Form and Function. Prevent, Treat and Maintain.
Sexual Function Problems
The vagina is all too commonly viewed as being in a ‘fixed’ state, described when there is a problem perceived about its dimensions as either too tight or too loose. Except in exceptional pathological states (induced by conditions such as atrophy and surgical or radiation induced tightness) the vagina is a dynamic organ. The dimensions and its responsiveness result from a complex interplay of psychological, neurological, emotional, hormonal, physical and environmental/social influences.
There may be up to a 50% reduction of the coital rate in the first year of marriage and a further 50% reduction after 20 years. The decline in sexual activity is greater for women than men of the same age, however about 1/3rd of women over 60 remain sexually active. The sharpest decline in sexual activity for women is at menopause.
What are sexual function problems?
- A departure from normal sensation &/or function experienced by a woman during sexual activity.
Dr Onuma has internationally recognised expertise in sexual dysfunction which has a physical basis. His approach involves:
- Making the right diagnosis
- Counselling and educating his patients so that they are involved in the care delivered
- Individually tailored surgery and non-surgical treatments
- Correct timing of treatments
The physical basis of female sexual dysfunction
- Painful intercourse
- Vaginal scar tissue
- Vaginal skin tags
- Labial elongation
- Endometriosis
- Interstitial cystitis
- Vaginal wall prolapse
- Uterine prolapse
- Reduced sensation
- Vaginal epithelial relaxation
- Vaginal wall prolapse
- Detached perineal body
- Clitoral hood hypertrophy
- Other conditions impacting on sexual function
- Vaginismus
- Urinary incontinence
- Appearance of external genitalia
- Vaginal flatus